
Volume 27, Issue 4 (1-2025)
jha 2025, 27(4): 67-83 |
Back to browse issues page

![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jani S, Mehara M, Khodadad Kashi F, Soleimani Y. Estimation of willingness to pay for the use of monkeypox vaccine in Iran. jha 2025; 27 (4) :67-83
URL: http://jha.iums.ac.ir/article-1-4413-en.html
URL: http://jha.iums.ac.ir/article-1-4413-en.html



1- Department of Economics, Payam Noor University, Tehran, Iran. , s.jani@pnu.ac.ir
2- Department of Economics, University of Tehran, Tehran, Iran.
3- Department of Economics, Payam Noor University, Tehran, Iran.
4- Payam Noor University, Tehran, Iran.
2- Department of Economics, University of Tehran, Tehran, Iran.
3- Department of Economics, Payam Noor University, Tehran, Iran.
4- Payam Noor University, Tehran, Iran.
Full-Text [PDF 1427 kb]
(26 Downloads)
| Abstract (HTML) (71 Views)
B i B i B i B i
Initially, one of the two prices is randomly selected, and the respondent is asked to express their willingness to pay in comparison to the proposed amount. After collecting consumer responses, the willingness to pay is then calculated (Figure 1).
Pre-test questionnaire:The primary objective of the pre-test questionnaire was to determine the bid amounts. Therefore, participants were first asked about their monthly expenses, followed by their net monthly income. Individuals reporting no income were excluded from the analysis. The main item in the pre-test questionnaire was an open-ended question regarding willingness to pay for a vaccine, which was used to determine initial bid values.Several methods exist for determining bid amounts; in this study, Cooper’s method [8], known as the “Bid Distribution with Equal Area Bid Selection (DWEABS)” was employed.
In their handbook on contingent valuation, Alberini and Kahn [11] suggested a sample size of 30 to 100 for pre-tests .Accordingly, 46 individuals participated in the pre-test to calculate the WTP for the monkeypox vaccine. The pre-test results indicated a right-skewed, asymmetric distribution of WTP bids. Therefore, logarithmic transformation was applied to the data. Some observations were excluded during transformation, reducing the sample size to 40 participants. The log-transformed WTP data followed a normal distribution, as confirmed by the Shapiro-Wilk test, indicating that the WTP bids derived from the pre-test questionnaire followed a log-normal distribution.
Based on the pre-test data, the coefficient of variation (CV) for the logarithm of WTP amounts was calculated as 1.4. Assuming a precision level (Δ) of 15% and using the t-statistic of 2.021 at a 5% significance level (α), for 40 observations, the required sample size was determined using the Mitchell and Carson formula (Equation 1) [7]. Accordingly, the required sample size was estimated at 356 participants, and the final survey was conducted online during the summer of 2023.
n t α CV 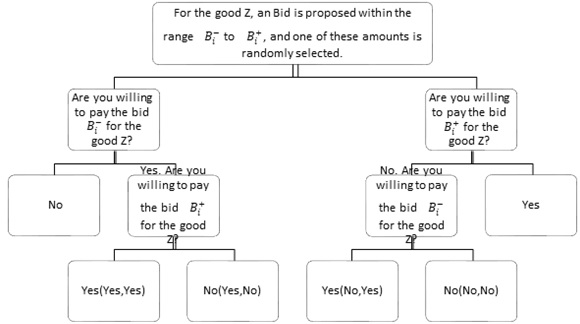
Figure 1. The one-and-one-half bound (OOHB) dichotomous choice method
WTP i Z i , u i Z i β u i t i Bid i y i WTP t i WTP t i Z i < WTP <
pr y = pr y , y = pr WTP > t 2 = pr Z i ' β + u i < t 2 = pr u i σ < t 2 σ - Z i ' β σ = G ( u i σ < t 2 1 σ - Z i ' β σ ) LnL OOHB θ = i =1 N d i y In 1- G u i σ < t 2 σ - Z i ' β σ + d i ny In G u i σ < t 2 σ - Z i ' β σ - G u i σ < t 1 σ - Z i ' β σ + d i n In G ( u i σ < t 1 σ - Z i ' β σ )
d i y ={ 1 if y , y , y WTP > t 2 0 ot h erwise & d i n ={ 1 if n , n , n WTP < t 1 0 ot h erwise
d i y ={ 1 if n , y , y , n t 1 < WTP < t 2 0 ot h erwise
Table 2. Mean, truncated mean at maximum bid, adjusted truncated mean at maximum bid, and median willingness to pay
Full-Text: (8 Views)
Introduction
One of the key concerns in economics is the pricing of goods and services, particulary in the medical field. Given the spread of infectious diseases and advancements in vaccine development, evaluating vaccine value from the consumers’ perspective is crucial for the effective implementation of preventive measures prior to outbreaks. Infectious diseases, depending on their type and transmission rate, pose serious threats to public health and may result in fatalities. Examples include plague, influenza, COVID-19, and smallpox, all of which have caused significant loss of lifes. Among these, smallpox and its variants continue to pose challenges for many societies. Prior to the 20th century, smallpox caused an estimated 300 to 540 million deaths worldwide [1]. Monkeypox is a viral infectious disease that affects humans and some certain animals. It may initially resemble influenza but later leads to rashes that progress to blisters and scabs, and in some cases, can be fatal [2].
The most common method for determining value is the equilibrium price, dervied from the intersection of supply and demand curves in the market. However, if vaccine pricing is determine solely by market forces, many individuals may be unable to afford it, making it impossible to prevent the spread of infectious diseases in society.
According to economic theory, the optimal level of production for goods with positive externalities is achieved when the sum of marginal private and external benefits equals the cost of production [3]. However, individuals typically consider only their private (individual) benefits when expressing demand for such goods, neglecting external (social) benefits. Consequently, without government intervention, the market equilibrium of production and consumption will fall short of the efficient level.
To date, no study in Iran has examined the willingness to pay for the monkeypox vaccine. However, related studies have been conducted in other countries, including those by Harapan et al. [4], Heng et al. [5], and Alrifai et al. [6] in 2023. Accordingly, this study employs the contingent valuation method using the one-and-one-half-bound (OOHB) dichotomous choice to estimate the willingness to pay for the monkeypox vaccine in Iran.Unlike many previous studies, this research increases precision and reliability by determining bid amount for willingness to pay through Cooper's method. This approach ensures full coverage under the probability distribution curve, thereby minimizing squared errors for willingness to pay. Finally, the study estimates willingness to pay across different segments of society, including various income groups, to provide more detailed insights and support effective planning by policymakers and pharmaceutical companies.
Methods
The study population was the entire country of Iran, and data were collected in the summer of 2023. The required information was gathered through a questionnaire. Random sampling was used, with the sample size determined using the Mitchell and Carson method [7], and bid amounts for willingness to pay were calculated using Cooper’s approach [8]. The questionnaire was administered online through the Parseline website. The questionnaire was distributed in two phases: a pre-test and the main questionnaire. Data analysis to estimate individuals’ willingness to pay was conducted using the contingent valuation method based on the one-and-a-half-bound dichotomous choice approach.
Contingent valuation (CV) is a survey-based method used to determine the values people assign to goods, services, and facilities [9]. The one-and-one-half-bound (OOHB) dichotomous choice method was introduced by Cooper et al. [10] to improve the accuracy of calculating individuals' willingness to pay in the contingent valuation method. This approach minimizes or eliminates discrepancies in survey responses. Respondents are shown a range or interval of proposed amounts
One of the key concerns in economics is the pricing of goods and services, particulary in the medical field. Given the spread of infectious diseases and advancements in vaccine development, evaluating vaccine value from the consumers’ perspective is crucial for the effective implementation of preventive measures prior to outbreaks. Infectious diseases, depending on their type and transmission rate, pose serious threats to public health and may result in fatalities. Examples include plague, influenza, COVID-19, and smallpox, all of which have caused significant loss of lifes. Among these, smallpox and its variants continue to pose challenges for many societies. Prior to the 20th century, smallpox caused an estimated 300 to 540 million deaths worldwide [1]. Monkeypox is a viral infectious disease that affects humans and some certain animals. It may initially resemble influenza but later leads to rashes that progress to blisters and scabs, and in some cases, can be fatal [2].
The most common method for determining value is the equilibrium price, dervied from the intersection of supply and demand curves in the market. However, if vaccine pricing is determine solely by market forces, many individuals may be unable to afford it, making it impossible to prevent the spread of infectious diseases in society.
According to economic theory, the optimal level of production for goods with positive externalities is achieved when the sum of marginal private and external benefits equals the cost of production [3]. However, individuals typically consider only their private (individual) benefits when expressing demand for such goods, neglecting external (social) benefits. Consequently, without government intervention, the market equilibrium of production and consumption will fall short of the efficient level.
To date, no study in Iran has examined the willingness to pay for the monkeypox vaccine. However, related studies have been conducted in other countries, including those by Harapan et al. [4], Heng et al. [5], and Alrifai et al. [6] in 2023. Accordingly, this study employs the contingent valuation method using the one-and-one-half-bound (OOHB) dichotomous choice to estimate the willingness to pay for the monkeypox vaccine in Iran.Unlike many previous studies, this research increases precision and reliability by determining bid amount for willingness to pay through Cooper's method. This approach ensures full coverage under the probability distribution curve, thereby minimizing squared errors for willingness to pay. Finally, the study estimates willingness to pay across different segments of society, including various income groups, to provide more detailed insights and support effective planning by policymakers and pharmaceutical companies.
Methods
The study population was the entire country of Iran, and data were collected in the summer of 2023. The required information was gathered through a questionnaire. Random sampling was used, with the sample size determined using the Mitchell and Carson method [7], and bid amounts for willingness to pay were calculated using Cooper’s approach [8]. The questionnaire was administered online through the Parseline website. The questionnaire was distributed in two phases: a pre-test and the main questionnaire. Data analysis to estimate individuals’ willingness to pay was conducted using the contingent valuation method based on the one-and-a-half-bound dichotomous choice approach.
Contingent valuation (CV) is a survey-based method used to determine the values people assign to goods, services, and facilities [9]. The one-and-one-half-bound (OOHB) dichotomous choice method was introduced by Cooper et al. [10] to improve the accuracy of calculating individuals' willingness to pay in the contingent valuation method. This approach minimizes or eliminates discrepancies in survey responses. Respondents are shown a range or interval of proposed amounts
Initially, one of the two prices is randomly selected, and the respondent is asked to express their willingness to pay in comparison to the proposed amount. After collecting consumer responses, the willingness to pay is then calculated (Figure 1).
Pre-test questionnaire:The primary objective of the pre-test questionnaire was to determine the bid amounts. Therefore, participants were first asked about their monthly expenses, followed by their net monthly income. Individuals reporting no income were excluded from the analysis. The main item in the pre-test questionnaire was an open-ended question regarding willingness to pay for a vaccine, which was used to determine initial bid values.Several methods exist for determining bid amounts; in this study, Cooper’s method [8], known as the “Bid Distribution with Equal Area Bid Selection (DWEABS)” was employed.
In their handbook on contingent valuation, Alberini and Kahn [11] suggested a sample size of 30 to 100 for pre-tests .Accordingly, 46 individuals participated in the pre-test to calculate the WTP for the monkeypox vaccine. The pre-test results indicated a right-skewed, asymmetric distribution of WTP bids. Therefore, logarithmic transformation was applied to the data. Some observations were excluded during transformation, reducing the sample size to 40 participants. The log-transformed WTP data followed a normal distribution, as confirmed by the Shapiro-Wilk test, indicating that the WTP bids derived from the pre-test questionnaire followed a log-normal distribution.
Based on the pre-test data, the coefficient of variation (CV) for the logarithm of WTP amounts was calculated as 1.4. Assuming a precision level (Δ) of 15% and using the t-statistic of 2.021 at a 5% significance level (α), for 40 observations, the required sample size was determined using the Mitchell and Carson formula (Equation 1) [7]. Accordingly, the required sample size was estimated at 356 participants, and the final survey was conducted online during the summer of 2023.
Figure 1. The one-and-one-half bound (OOHB) dichotomous choice method
Main questionnaire: The main questionnaire, designed to achieve the study objectives and examine individuals’ preferences and willingness to pay, was developed in two sections: the first section covered socioeconomic variables, while the second focused on willingness to pay for the monkeypox vaccine. Based on the pre-test data, two bid ranges were selected: 65,000 to 117,000 Iranin Tomans (IRT) and 117,000 to 212,000 (Tomans). One of these amounts was randomly offered to each respondent.
The model:To examine the factors influencing the WTP for the monkeypox vaccine, the following model (Equation 2) was considered.
The model:To examine the factors influencing the WTP for the monkeypox vaccine, the following model (Equation 2) was considered.
The probability of responses of "No-Yes" and "Yes-
No" is expressed in Equation (4) as follows:
No" is expressed in Equation (4) as follows:
The probability of responses of "Yes" and "Yes-
Yes" is expressed in Equation (5) as follows
Yes" is expressed in Equation (5) as follows
The maximum likelihood function is expressed in
Equation (6) as follows:
Equation (6) as follows:
Results
To estimate willingness to pay based on the valuation method, it is first necessary to collect and analyze the data using the questionnaire described in the previous section. The one-and-one-half-bounded model was estimated using the maximum likelihood method in RStudio software [12,13]. The estimation results are presented in Table 1.
Table 1. Estimation of the one-and-one-half bound model
To estimate willingness to pay based on the valuation method, it is first necessary to collect and analyze the data using the questionnaire described in the previous section. The one-and-one-half-bounded model was estimated using the maximum likelihood method in RStudio software [12,13]. The estimation results are presented in Table 1.
Table 1. Estimation of the one-and-one-half bound model
| Probability value | Z test statistic | Standard error | Estimated coefficients | Variables | |
| 1.786635 | 0.000317*** | 3.6009 | 1.0506 | 3.7832 | Intercept |
| 0.241865 | 0.000021*** | 4.2516 | 0.1226 | 0.5213 | Age |
| 0.1324203 | 0.235987 | 1.1851 | 0.2366 | 0.2804 | Gender |
| 0.0922314 | 0.395463 | 0.8498 | 0.2298 | 0.1953 | Marital status |
| 0.2187485 | 0.013979* | 2.4578 | 0.1885 | 0.4632 | Education level |
| 0.3046517 | 0.000193*** | 3.7286 | 0.1730 | 0.6451 | Income |
| 0.2356553 | 0.026678* | 2.2162 | 0.2251 | 0.4990 | Disease background |
| 0.2526092 | 0.032920* | 2.1331 | 0.2508 | 0.5349 | Importance to health issues |
| 1 | 0.000000*** | -10.509 | 0.2015 | -2.1175 | log(bid) |
| Significance codes: 0 ‘***’ 0.001 ‘**’ 0.01 ‘*’ 0.05 ‘.’ 0.1 ‘ ’ 1 | |||||
| Distribution: Log-logistic Number of Observations: 356 Log-Likelihood: -313.057149 Likelihood Ratio: 107.961 with 8 degrees of freedom, p-value = 0.000 Akaike Information Criterion (AIC): 644.114298 Bayesian Schwarz Criterion (BIC): 678.988675 | |||||
As shown by the reported significance levels, the logarithm of the bid amount is statistically significant. Additionally, based on the Akaike Information Criterion (AIC) and the Bayesian Schwarz Criterion (BIC), among the five considered error term distributions (normal, log-normal, logistic, log-logistic, and Weibull), the log-logistic distribution was selected.
To interpret the model estimates, the coefficients were transformed using the formulaβ
According to the reported significance levels, the variables that significantly affect willingness to pay include age, education, income, disease background, and importance to health issues. The effect of education on willingness to pay is positive and statistically significant, as theoretically expected, indicating that individuals with higher education levels are more willing to pay for the monkeypox vaccine. Specifically, a one-level increase in education leads to 21% increase in individuals’ willingness to pay. Similarly, the coefficient for “income” is positive and significant, indicating that a one-level increase in income leads to a 30% increase in the willingness to pay for the monkeypox vaccine. “Disease background” also shows the expected positive sign, suggesting that individuals with such conditions have a higher willingness to pay. Having a disease background increases willingness to pay for the monkeypox vaccine by 23%.
According to Table 1, the estimated coefficient for “importance to health issues” shows that individuals who consider health matters important are more willing to pay for the monkeypox vaccine. Therefore, lifestyle changes and greater concern for health increase the probability of willingness to pay by approximately 25%. Regarding age, the findings indicate that a one-level increase in age results in a 24% increase in willingness to pay for the monkeypox vaccine.
To interpret the model estimates, the coefficients were transformed using the formula
According to the reported significance levels, the variables that significantly affect willingness to pay include age, education, income, disease background, and importance to health issues. The effect of education on willingness to pay is positive and statistically significant, as theoretically expected, indicating that individuals with higher education levels are more willing to pay for the monkeypox vaccine. Specifically, a one-level increase in education leads to 21% increase in individuals’ willingness to pay. Similarly, the coefficient for “income” is positive and significant, indicating that a one-level increase in income leads to a 30% increase in the willingness to pay for the monkeypox vaccine. “Disease background” also shows the expected positive sign, suggesting that individuals with such conditions have a higher willingness to pay. Having a disease background increases willingness to pay for the monkeypox vaccine by 23%.
According to Table 1, the estimated coefficient for “importance to health issues” shows that individuals who consider health matters important are more willing to pay for the monkeypox vaccine. Therefore, lifestyle changes and greater concern for health increase the probability of willingness to pay by approximately 25%. Regarding age, the findings indicate that a one-level increase in age results in a 24% increase in willingness to pay for the monkeypox vaccine.
Table 2. Mean, truncated mean at maximum bid, adjusted truncated mean at maximum bid, and median willingness to pay
| Simulated confidence intervals using the bootstrap method | Simulated confidence intervals using the Krinsky and Rob method | ||||
| Upper bound | Lower bound | Upper bound | Lower bound | Estimates | Estimation of willingness to pay |
| 164.04 | 115.547 | 165.02 | 119.493 | 136.1201 | Mean |
| 114.56 | 96.289 | 113.11 | 98.246 | 105.8674 | Truncated mean at maximum bid |
| 139.38 | 107.412 | 136.94 | 111.638 | 123.6931 | Adjusted truncated mean at maximum bid |
| 102.82 | 79.021 | 100.91 | 81.398 | 91.40098 | Median |
Table 2 presented the simulated intervals obtained using the Krinsky and Rob method [14,15], as well as the bootstrap method.. According to Table 2, the median is 91,000 Tomans, while the mean is 136,000 Tomans. Truncated mean at maximum bid is 105,000 Tomans, and adjusted truncated mean at maximum bid is 123,000 Tomans.
Table 3. Mean and median willingness to pay for different levels of a variable
| Upper bound | Lower bound | Estimates | Statistics | Level | Variable |
| 151.642 | 102.391 | 120.751 | Mean | No | Disease background |
| 96.006 | 67.871 | 81.081 | Median | ||
| 194.95 | 127.906 | 152.837 | Mean | Yes | |
| 116.94 | 87.979 | 10.626 | Median | ||
| 141.83 | 80.499 | 103.139 | Mean | Below average (careless) | Importance to health issues |
| 92.42 | 51.362 | 69.255 | Median | ||
| 166.472 | 116.163 | 132.781 | Mean | Average (normal) | |
| 99.313 | 78.657 | 89.159 | Median | ||
| 234.02 | 133.761 | 170.941 | Mean | Above average (sensitive) | |
| 142.97 | 91.178 | 114.782 | Median | ||
| 113.642 | 62.915 | 81.875 | Mean | Below 5 million |
Income in Tomans |
| 74.138 | 40.741 | 54.976 | Median | ||
| 138.314 | 93.961 | 111.036 | Mean | 5 to 10 million |
|
| 86.381 | 61.944 | 74.558 | Median | ||
| 188.89 | 129.692 | 150.584 | Mean | 10 to 15 million |
|
| 113.53 | 88.891 | 101.113 | Median | ||
| 285.16 | 155.94 | 204.22 | Mean | 15 to 20 million |
|
| 167.04 | 108.06 | 137.13 | Median | ||
| 467.24 | 187.22 | 276.96 | Mean | Over 20 million |
|
| 280.38 | 123.62 | 185.97 | Median |
Table 3 presnets mean and median of willingness to pay across different groups, including disease background, importance to health issues, and income. Tthe willingness to pay for income groups below 5 million, 50 to 10 million, 10 to 15 million, 15 to 20 million and and above 20 million Tomans were 81,000, 111,000, 150,000, 204,000, and 276,000 Tomans, respectively. Additionally, people without a disease background have an average willingness to pay of 120,000 Tomans, while those with a disease background tend to pay around 152,000 Tomans on average. The estimation of willingness to pay at three levels of “importance to health issues” also showed that the average willingness to pay increases with increasing importance of health issues for participants. Specifically, individials categorized as careless, normal and sensitive tend to pay 103,000, 132,000 and 170,000 Tomans, respectively.
Discussion
This study investigated the willingness to pay for the monkeypox vaccine among the Iranian population and found that the median and mean willingness to pay for the monkeypox vaccine were estimated at 91,000 and 136,000 Tomans, respectively. Therefore, it can be concluded that during the early stages of the outbreak of this disease, subsidies could encourage many individuals to use the monkeypox vaccine and prevent fatalities. It is worth noting that, compared to other studies, the willingness to pay for the monkeypox vaccine in Iran (about 2.5 USD or 136,000 Tomans) is lower than the willingness to pay reported in other studies, such as Indonesian physicians (approximately 37 USD) [4], and Vietnamese people (about 8 USD) [16].
According to the present study, the variables affecting willingness to pay for the monkeypox vaccine in Iran included age, education, income, disease background, and importance to health issues. On the other hand, gender and marital status did not show a significant relationship with willingness to pay for the monkeypox vaccine. These findings align largly with the study by Harapan et al. [4], which examined factors influencing willingness to pay for monkeypox vaccines among Indonesian physicians. It demonstrated that factors such as medical experience duration and monthly income affect willingness to pay for the vaccine. Additionally, our findings are consistent with those of Hong et al. [5] and Elrifi et al. [6]. In Elrifi et al.'s study, previous vaccination history (such as influenza and COVID-19) was significantly associated with willingness to get vaccinated for Mpox, while gender, marital status and nationality did not significantly influence the willingness to get vaccinated. Similarly, Hong et al. [5] found that Chinese people to receive vaccination was mainly correlated to age, hospital level, and attitude toward vaccination. Overall, this study indicates that designing effective vaccination policies in Iran requires consideration of both economic and psychological factors. Relying solely on market-based pricing cannot ensure adequate vaccination coverage.
Limitations
This study has two limitations that may have influenced the results. First, the use of an online questionnaire excluded certain segments of the population who lacked adequate internet access or the skills to use it, including the elderly, individuals with lower levels of education, and those living in rural or underserved areas. Second, the context of the early outbreak and the level of public awareness or concern at the time of data collection (summer 2023) may have affected responses. Consequently, the results could vary under different circumstances. Therefore, these limitations should be considered when analyzing and interpreting the findings.
Conclusion
This study examined the willingness to pay (WTP) for the monkeypox vaccine among the Iranian population using the contingent valuation method based on the one-and-one-half-bounded (OOHB) dichotomous choice approach. The study found that the average WTP for the monkeypox vaccine in Iran is 136,000 Tomams, an amount lower than the actual cost of production and distribution of the vaccine in the market, which is estimated to be between 211,000 and 216,000 Tomans. This gap between individuals' perceived value and the real market price underscores the necessity for government intervention through supportive policies. Furthermore, variables such as age, education level, income, disease background, and importance to health issues were found to have a significant positive impact on WTP. In contrast, gender and marital status did not show a significant effect. These findings suggest that psychological, economic, and health-related factors play a more substantial role in shaping individual behavior than purely demographic characteristics.
Based on these findings, the following multidimensional policy recommendations can be proposed for policymakers, pharmaceutical companies, and public health institutions: 1) Targeted subsidy-based policies: it is recommended that the government implement tiered, income-based subsidies to cover vaccination costs. Such policies could promote greater equity in access and maximize vaccination coverage, especially among vulnerable and low-income groups who demonstrate lower willingness to pay. 2) Raising awareness and shifting public attitudes: given the importance of health attitudes in WTP, it is suggested that large-scale national education and information campaigns be launched. These should focus on the consequences of monkeypox, vaccine effectiveness, and the importance of prevention. Such efforts can enhance actual WTP by increasing risk perception and awareness of vaccination benefits. 3) Implications for pricing and production planning: the findings can be particularly useful for pharmaceutical companies and vaccine manufacturers. A better understanding of consumers’ acceptable maximum price can help these firms plan more effectively for production, distribution, and marketing strategies. 4) Gradual and region-specific vaccination programs: since demographic factors such as health history and income vary across regions, implementing regional and data-driven policies can enhance the efficiency of vaccination programs. 5) Planning for future emergencies: this study also provides an indirect framework for quicker, evidence-based responses during outbreaks of other infectious diseases. Early insights into WTP can guide the design of rapid intervention packages in the initial stages of an epidemic.
In conclusion, this research marks an important first step toward understanding the economic and behavioral dimensions of monkeypox vaccine uptake in Iran. Continued research on other diseases, dynamic assessments over time, and integration of quantitative and qualitative methods can pave the way for the development of smart, effective, and equitable public health policies in the country.
Supplement: Questionnaires
Declarations:
Ethical Considerations: This article is derived from a dissertation titled “estimation of willingness to pay for vaccines for contagious diseases (Influenza and Monkeypox) using the contingent valuation method, as part of a doctoral program in Economics at the Graduate Studies Center of Payame Noor University in Tehran. All ethical principles have been respected in this research.
Funding: This study has been conducted without any financial support.
Conflict of Interest: The authors declare that there is no conflict of interest.
Author Contributions: Siavash Jani: Study design, data curation, data analysis, writing– original draft, final approval; Mohsen Mehara: Study design, data curation, data analysis, final approval; Farhad Khodadadkashi: Study design, data curation, final approval; Yasha Soleimani: Study design, data curation, data analysis, software, writing– original draft, final approval.
Consent for Publication: None.
Data Availability: The data used in this study is available at the Data Monkeypox link.
Use of Artificial Intelligence: The authors used ChatGPT-4.0 artificial intelligence to edit the grammar of the text.
Acknowledgments: The authors express their gratitude to all individuals who collaborated in this research.This published article is part of a doctoral dissertation entitled "The estimation of willingness to pay for vaccines against contagious diseases (influenza and monkeypox) using the contingent valuation method." approved in 2023 by Department of Tehran Graduate Studies Center of Payame Noor University, Tehran, with the code D/32/19750.
Discussion
This study investigated the willingness to pay for the monkeypox vaccine among the Iranian population and found that the median and mean willingness to pay for the monkeypox vaccine were estimated at 91,000 and 136,000 Tomans, respectively. Therefore, it can be concluded that during the early stages of the outbreak of this disease, subsidies could encourage many individuals to use the monkeypox vaccine and prevent fatalities. It is worth noting that, compared to other studies, the willingness to pay for the monkeypox vaccine in Iran (about 2.5 USD or 136,000 Tomans) is lower than the willingness to pay reported in other studies, such as Indonesian physicians (approximately 37 USD) [4], and Vietnamese people (about 8 USD) [16].
According to the present study, the variables affecting willingness to pay for the monkeypox vaccine in Iran included age, education, income, disease background, and importance to health issues. On the other hand, gender and marital status did not show a significant relationship with willingness to pay for the monkeypox vaccine. These findings align largly with the study by Harapan et al. [4], which examined factors influencing willingness to pay for monkeypox vaccines among Indonesian physicians. It demonstrated that factors such as medical experience duration and monthly income affect willingness to pay for the vaccine. Additionally, our findings are consistent with those of Hong et al. [5] and Elrifi et al. [6]. In Elrifi et al.'s study, previous vaccination history (such as influenza and COVID-19) was significantly associated with willingness to get vaccinated for Mpox, while gender, marital status and nationality did not significantly influence the willingness to get vaccinated. Similarly, Hong et al. [5] found that Chinese people to receive vaccination was mainly correlated to age, hospital level, and attitude toward vaccination. Overall, this study indicates that designing effective vaccination policies in Iran requires consideration of both economic and psychological factors. Relying solely on market-based pricing cannot ensure adequate vaccination coverage.
Limitations
This study has two limitations that may have influenced the results. First, the use of an online questionnaire excluded certain segments of the population who lacked adequate internet access or the skills to use it, including the elderly, individuals with lower levels of education, and those living in rural or underserved areas. Second, the context of the early outbreak and the level of public awareness or concern at the time of data collection (summer 2023) may have affected responses. Consequently, the results could vary under different circumstances. Therefore, these limitations should be considered when analyzing and interpreting the findings.
Conclusion
This study examined the willingness to pay (WTP) for the monkeypox vaccine among the Iranian population using the contingent valuation method based on the one-and-one-half-bounded (OOHB) dichotomous choice approach. The study found that the average WTP for the monkeypox vaccine in Iran is 136,000 Tomams, an amount lower than the actual cost of production and distribution of the vaccine in the market, which is estimated to be between 211,000 and 216,000 Tomans. This gap between individuals' perceived value and the real market price underscores the necessity for government intervention through supportive policies. Furthermore, variables such as age, education level, income, disease background, and importance to health issues were found to have a significant positive impact on WTP. In contrast, gender and marital status did not show a significant effect. These findings suggest that psychological, economic, and health-related factors play a more substantial role in shaping individual behavior than purely demographic characteristics.
Based on these findings, the following multidimensional policy recommendations can be proposed for policymakers, pharmaceutical companies, and public health institutions: 1) Targeted subsidy-based policies: it is recommended that the government implement tiered, income-based subsidies to cover vaccination costs. Such policies could promote greater equity in access and maximize vaccination coverage, especially among vulnerable and low-income groups who demonstrate lower willingness to pay. 2) Raising awareness and shifting public attitudes: given the importance of health attitudes in WTP, it is suggested that large-scale national education and information campaigns be launched. These should focus on the consequences of monkeypox, vaccine effectiveness, and the importance of prevention. Such efforts can enhance actual WTP by increasing risk perception and awareness of vaccination benefits. 3) Implications for pricing and production planning: the findings can be particularly useful for pharmaceutical companies and vaccine manufacturers. A better understanding of consumers’ acceptable maximum price can help these firms plan more effectively for production, distribution, and marketing strategies. 4) Gradual and region-specific vaccination programs: since demographic factors such as health history and income vary across regions, implementing regional and data-driven policies can enhance the efficiency of vaccination programs. 5) Planning for future emergencies: this study also provides an indirect framework for quicker, evidence-based responses during outbreaks of other infectious diseases. Early insights into WTP can guide the design of rapid intervention packages in the initial stages of an epidemic.
In conclusion, this research marks an important first step toward understanding the economic and behavioral dimensions of monkeypox vaccine uptake in Iran. Continued research on other diseases, dynamic assessments over time, and integration of quantitative and qualitative methods can pave the way for the development of smart, effective, and equitable public health policies in the country.
Supplement: Questionnaires
Declarations:
Ethical Considerations: This article is derived from a dissertation titled “estimation of willingness to pay for vaccines for contagious diseases (Influenza and Monkeypox) using the contingent valuation method, as part of a doctoral program in Economics at the Graduate Studies Center of Payame Noor University in Tehran. All ethical principles have been respected in this research.
Funding: This study has been conducted without any financial support.
Conflict of Interest: The authors declare that there is no conflict of interest.
Author Contributions: Siavash Jani: Study design, data curation, data analysis, writing– original draft, final approval; Mohsen Mehara: Study design, data curation, data analysis, final approval; Farhad Khodadadkashi: Study design, data curation, final approval; Yasha Soleimani: Study design, data curation, data analysis, software, writing– original draft, final approval.
Consent for Publication: None.
Data Availability: The data used in this study is available at the Data Monkeypox link.
Use of Artificial Intelligence: The authors used ChatGPT-4.0 artificial intelligence to edit the grammar of the text.
Acknowledgments: The authors express their gratitude to all individuals who collaborated in this research.This published article is part of a doctoral dissertation entitled "The estimation of willingness to pay for vaccines against contagious diseases (influenza and monkeypox) using the contingent valuation method." approved in 2023 by Department of Tehran Graduate Studies Center of Payame Noor University, Tehran, with the code D/32/19750.
Type of Study: Research |
Subject:
Health Economics
Received: 2024/12/18 | Accepted: 2024/07/15 | Published: 2025/07/27
Received: 2024/12/18 | Accepted: 2024/07/15 | Published: 2025/07/27
Supplement 1 [PDF 709 KB] (4 Download)
Supplement 2 [PDF 490 KB] (4 Download)
References
1. Selgelid MJ. Smallpox revisited?. American Journal of Bioethics. 2003 ; 3(1):5-11. doi: [DOI:10.1162/152651603322781620]
2. "WHO Factsheet - Mpox (Monkeypox)". World Health Organization (WHO). 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/mpox
3. Guardian Council. The Constitution of the Islamic Republic of Iran. Available from: https://www.shora-gc.ir/files/fa/news/1398/9/21/4354_236.pdf
4. Pezhoyan J . Public Sector Economics (Costs). Jangal Publications, 8th edition, 2010. p. 129. [In Persian]
5. Harapan H, Wagner AL, Yufika A, Setiawan AM, Anwar S, Wahyuni S. Acceptance and willingness to pay for a hypothetical vaccine against monkeypox viral infection among frontline physicians: a cross-sectional study in Indonesia. Vaccine. 2020;38(43):6800-6. doi: [DOI:10.1016/j.vaccine.2020.08.034]
6. Hong J, Pan B, Jiang HJ, Zhang QM, Xu XW, Jiang H. The willingness of Chinese healthcare workers to receive monkeypox vaccine and its independent predictors: a cross‐sectional survey. Journal of Medical Virology. 2023;95(1):e28294. doi: [DOI:10.1002/jmv.28294]
7. Alarifi AM, Alshahrani NZ, Sah R. Are Saudi healthcare workers willing to receive the monkeypox virus vaccine? evidence from a descriptive-baseline survey. Tropical Medicine and Infectious Disease. 2023;8(8):396. doi: [DOI:10.3390/tropicalmed8080396]
8. Mitchell RC, Carson RT. Using surveys to value public goods: the contingent valuation method. Resources for the Future; 1989.
9. Cooper JC. Optimal bid selection for dichotomous choice contingent valuation surveys. Journal of Environmental Economics and Management.;24(1):25-40. doi: [DOI:10.1006/jeem.1993.1002]
10. Kjaer T. A review of the discrete choice experiment-with emphasis on its application in health care. Denmark: Syddansk Universitet; 2005. Available from: https://www.researchgate.net/publication/265363271_A_review_of_the_Discrete_Choice_Experiment-with_Emphasis_on_Its_Application_in_Health_Care
11. Boyle KJ. Contingent valuation in practice. in, PA Champ, KJ Boyle, TC Brown, eds., A primer on nonmarket valuation. 2003. Available from: [DOI:10.1007/978-94-007-7104-8_4]
12. Bishop RC, Heberlein TA. Measuring values of extramarket goods: Are indirect measures biased?. American Journal of Agricultural Economics. 1979;61(5):926-30. doi: [DOI:10.2307/3180348]
13. Kanninen BJ. Optimal experimental design for double-bounded dichotomous choice contingent valuation. Land Economics. 1993:138-46. doi: [DOI:10.2307/3146514]
14. Cooper JC, Hanemann M, Signorello G. One-and-one-half-bound dichotomous choice contingent valuation. Review of Economics and Statistics. 2002;84(4):742-50.doi: [DOI:10.1162/003465302760556549]
15. Hanemann WM. Welfare evaluations in contingent valuation experiments with discrete responses. American Journal of Agricultural Economics. 1984;66(3):332-41. doi: [DOI:10.2307/1240800]
16. Seller C, Stoll JR, Chavas JP. Validation of empirical measures of welfare change: a comparison of nonmarket techniques. Land Economics. 1985;61(2):156-75. doi: [DOI:10.2307/3145808]
17. Boyle KJ, Welsh MP, Bishop RC. Validation of empirical measures of welfare change: Comment. Land Economics. 1988;64(1):94-8. doi: [DOI:10.2307/3146613]
18. Krinsky I, Robb AL. On approximating the statistical properties of elasticities. the review of economics and statistics. 1986 1:715-9. doi: [DOI:10.2307/1924536]
19. Krinsky I, Robb AL. On approximating the statistical properties of elasticities: A correction. Review of Economics & Statistics. 1990;72(1):189-90. [DOI:10.2307/1924536]
20. Alberini A, Kahn J. Handbook on contingent valuation. Edward Elgar Publishing; 2006. [DOI:10.4337/9781845427917]
21. Aizaki H, Nakatani T, Sato K. Stated preference methods using R. CRC Press; 2014. [DOI:10.1201/b17292]
22. Aizaki H, Nakatani T, Sato K, Fogarty J. R package DCchoice for dichotomous choice contingent valuation: a contribution to open scientific software and its impact. Japanese Journal of Statistics and Data Science. 2022 Dec;5(2):871-84. doi: [DOI:10.1007/s42081-022-00171-1]
23. Tran BX, Do LA, Hoang TP, Boyer L, Auquier P, Fond G. Crucial choices in a global health crisis: Revealing the demand and willingness to pay for a hypothetical monkeypox vaccine-the PREVENT study. Journal of Global Health. 2023;13.04033. doi: [DOI:10.7189/jogh.13.04033]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Site Keywords
Health, Administration, Scientific Article, Iran University of Medical Sciences,
